Hixny and Healthy Alliance make social support referrals easier for clinicians.
“The focus of our partnership is to support those working with the underserved, especially our clinical partners. We’re removing complexity and barriers for them. In the past, they didn’t want to ask about food or housing situations because they couldn’t solve those needs—they didn’t know what to do or to whom to refer the patient,” says Lynne Olney, Chief Transformation Officer at Healthy Alliance. “What our work with Hixny does is allow providers to ask about the situation a patient may be in, knowing they have a way to get them help if needed.”
This year, Hixny teamed up with Healthy Alliance to write a first-of-its-kind grant to integrate social determinants of health (SDoH) data alongside clinical data through a referral capability embedded within the patient record snapshot. Taking it one step further, once a referral has been made, the SDoH data is captured and integrated fully into the patient’s record. This means providers seen after the referral is made are aware that their patient may have unmet social needs impacting their health.
The focus of our partnership is to support those working with the underserved, especially our clinical partners. We’re removing complexity and barriers for them.
The goal of the project was to make it easy for a primary care clinician, an emergency room staff member, or anyone in between to identify a patient’s SDoH need and make a referral for social support. Providers can select a specific organization or refer the patient to Healthy Alliance’s referral coordination center for assistance, determining what care—and where—will be most helpful.
“We provide the referral coordination center as a service to providers,” explains Healthy Alliance CEO Erica Coletti. “There are lots of changing variables in the social space where the landscape of programs and services frequently changes in terms of availability, eligibility and geography. We want to take the navigation work across this complex environment off the clinician so they can focus on their interaction with the patient.”
Both Olney and Coletti agree that the biggest challenge, for their part, is ensuring that clinicians understand and convey to patients what will happen after the referral is made. This ensures patients are aware that they may be contacted by Healthy Alliance to help determine what steps to take and what organizations to involve most meet the patient’s needs.
We want to take the navigation work across this complex environment off the clinician so they can focus on their interaction with the patient.
Social Referrals for the Most Vulnerable Patients
For one care coordinator, using Hixny’s social referral tool was an easy choice.
“It’s so convenient! I can create a referral in a fraction of the time it took through our existing system,” they said. “We used to have a family support worker to do this, but now I do it myself, and Hixny really helped with that workflow.”
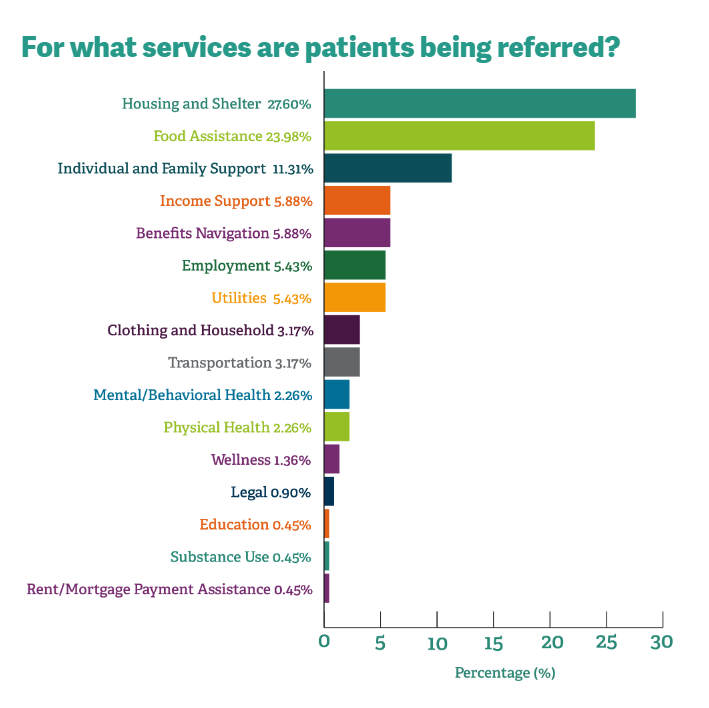
For this coordinator, whose patients are pregnant women who most often benefit from referrals to financial, day care or mental and behavioral health services, the opportunity to ask SDoH questions during intake, while reviewing clinical information, opens the door to broader conversations about their health.
“I love Hixny because I can find out so much about patients that I can’t find anywhere else,” they added. “I use it all the time!”
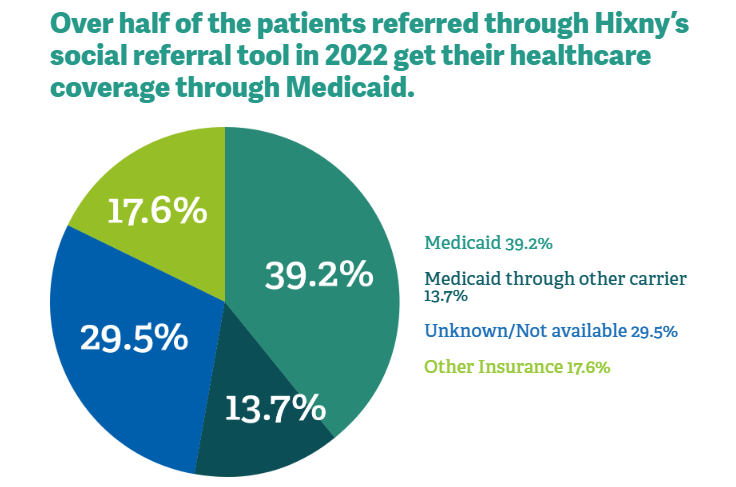
Alison Levine, LMSW, an OBGYN Social Worker at Albany Medical Center, works with a similar population. “I’m really grateful this tool exists,” she says. “It’s very helpful. The grant I’m working under focuses primarily on patients with Medicaid. Most are looking for SNAP (Supplemental Nutrition Assistance Program) benefits, help with rent, housing, utilities, or clothing and supplies for themselves and their baby.”
“There are a variety of things I can connect patients with,” Levine adds. “I didn’t know what agency offered what. The option to select submitting a request to the referral coordination center allows me to connect my patients to someone who can help with whatever they need.”
Onward to Integrated Outcomes Data
For Levine and other providers using the social referral tool, the only challenge is the ability to see that the referral led to the patient receiving assistance. At present, the system at the foundation of the referral tool does not connect to Hixny to close that loop, but not for lack of trying. As Healthy Alliance leaders point out, there are complicated contracts on the social care side of the equation that make it harder to connect those organizations than to connect clinical providers.
“A lot of outcomes data is currently in patient stories, so it’s more qualitative than quantitative and tied to health and well-being. It’s the personal interactions and whether the patient feels they got some help in addressing a challenge and what impact that help had,” explains Healthy Alliance’s Olney. “It’s perception more than data, but the patient’s perception of well-being is as much an outcome as clinical or numeric data.”
“Today, the process requires manual intervention,” Coletti says. “A key part of the process is showing the closed loop to the provider. As the provider asked the patient what they need and initiated a referral, they want to know the outcome of that connection. Currently, we are able to provide information manually on when the referral is closed and whether it was completed successfully or not and why. Removing the manual nature of this process is possible but requires the referral platform to be interoperable in a scalable way. In the meantime, Healthy Alliance and Hixny are committed to working through technical and policy barriers to make this process not only easy for the providers, but also the outcomes of the process visible to providers.”
