
Letter from the CEO
As Hixny celebrates 25 years of breaking down barriers across the healthcare ecosystem, we find ourselves at an inflection point in the industry. Recognition of the growing need for data and information is finally permeating mainstream thinking.
Healthcare technology has to change to meet this demand—and while it’s always lagged other industries, it’s catching up. It’s a unique field where care and contemplation in growth are required to avoid negatively affecting patients with an overly ambitious change.
Hixny is uniquely poised to meet the need, having shown a tremendous amount of leadership. By identifying developing trends, responding with meaningful solutions, and incrementally evolving our processes and capabilities toward maturity, we’ve built our services with an eye toward the future. And we continue to do so. Our expectation is not that we can rely on past accomplishments, but that each step takes us further down an infinite path.
And it’s working. Over the past few years, we’ve seen real progress in the way Hixny is used and we are confident the foundation we’ve built can help us achieve the next level of information delivery.
We’re already looking beyond the day-to-day, nuts-and-bolts connections to learn what people truly want when they seek information. We have an eye toward where we’re going.
Hixny has been executing that vision for a quarter century, and we’ll keep moving toward it in the future.

A Moment in Time: Hixny’s 25th Year
A quarter century ago, when Paul Macielak, then president and CEO of the New York Health Plan Association, and Gary Fitzgerald, then president and CEO of the Iroquois Healthcare Alliance, put their heads together to dream up what would become Hixny, their purpose was to bring hospitals and health plans to the table to improve the promptness of reimbursement for care.
No sooner had HIPAA been raised as a potential barrier to information sharing than the group became aware of a parallel consortium of local healthcare information officers working to solve that problem. Naturally, the groups merged efforts.
Yet trust remained elusive for nearly 20 years. Hixny’s original governance structure reflected that reality, allocating equal board seats to subgroups within the healthcare community, and requiring all parties to demonstrate that they had skin in the game in the form of dues. Earning trust led to greater flexibility and the introduction of consumer voices.
Macielak chalks up the extraordinary reshaping of the local healthcare landscape to Hixny’s only two CEOs: Dominick Bizarro, who served from 2007 to 2011, and Mark McKinney, who has held the role since Bizarro left in 2011. From creating a workable platform, to navigating changes in state and federal direction, to the revolutionary introduction of an EHR-embedded health information exchange (HIE) app, Hixny owes its longevity and growth to these two leaders.
Working Within the Workflow
Yet, New York’s Medicaid 1115 waiver program and similar initiatives still assume that HIEs are unsophisticated systems that simply replace sending files back and forth.
And for much of its history, Hixny served exactly that rudimentary purpose. Like our peers around the state and country, we were in an uphill battle to engage providers in using the HIE, when the technology existed outside routine, longstanding workflows.
Initially, we addressed this challenge by using web services to share standardized medical documents—Consolidated-Clinical Document Architecture (C-CDA)—with providers through their EHRs. This method proved cumbersome, due to the file size of C-CDAs, unextractable information, and limitations on searchability, among other factors. And still, providers had to summon and sort the data.
All that changed in 2020, when Hixny finally cracked the code to offering meaningful, actionable, individual information within provider workflows—and catapulted itself light years ahead in the quest to supersede the connection of systems and actively impact patient care.
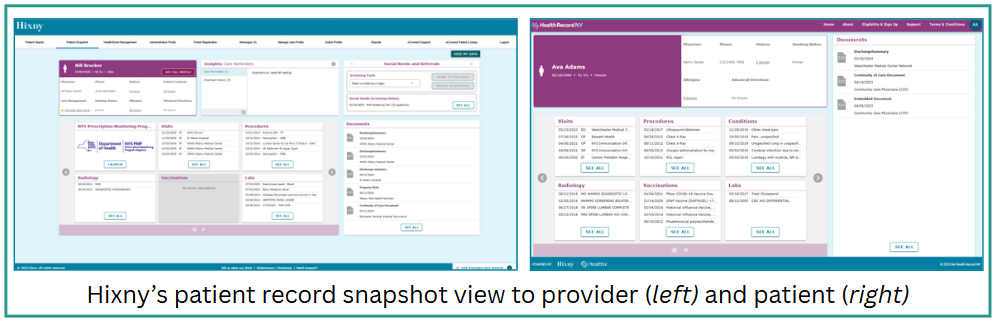
The Patient Record Snapshot
The emergence of Substitutable Medical Applications, Reusable Technologies (SMART) on Fast Healthcare Interoperability Resources (FHIR) technology created an alternative to C-CDAs. It allowed Hixny to truly integrate into a provider’s EHR workflow with no barriers.
Hixny’s snapshot has its own tab within the EHR interface, with its own app embedded on that tab, populating relevant information on the patient the provider is working with.
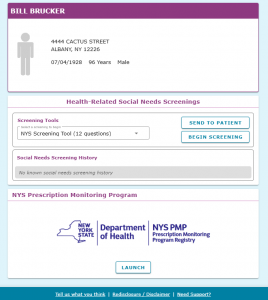
We decide what information is displayed and how it’s formatted, making relevant data more accessible to providers. The snapshot identifies itself as a Hixny app, so providers know where the information is coming from—and it prioritizes actionable care quality measures for providers. They can see at a glance if their patient needs a mammogram or colorectal cancer screening, for example.
Since launching, the snapshot has been augmented with a state-compliant health-related social needs (HRSN) assessment and accompanying referral tool. It’s seen upgrades in the number and nuances of insights called out as action items. And it’s successfully served up links to robust patient histories, labs, images, and notes in millions of patient visits.
Providers have accessed patient information through Hixny more than they ever did before the snapshot launched—by factors of 10. And they’re using it to find information that isn’t even available in C-CDAs.
Our Focus on Quality
What makes this all work is dedication to sharing high-quality data. Dedication that may start with Hixny, but permeates the facilities, practices, and organizations contributing the data that informs our insights.
Matching data to the correct patient is just the start. We work with our contributors to determine:
- How well does the data reflect what’s actually going on with the patient?
- Is the data up-to-date and does it reflect the patient’s current state?
- Are data values consistent across sources?
- Is the data the same across systems?
- Did the EHR send a complete patient record through the HIE?
- Does the data make sense for that patient (e.g., does a child’s health data describe a condition only present in geriatric patients)?
- Does the data meet the NCQA standards to be used for annual HEDIS reporting?
The range of data has changed with time, too. Patient data is integrated from pharmacies, community-based organizations and skilled nursing facilities; institutional, public health and government sources; and even patients using self-monitoring devices like at-home blood pressure cuffs and personal blood sugar meters. In some cases, like that of the state prescription monitoring program, we’ve integrated the display of important information into the snapshot, rather than bringing protected data into our own feeds.
This Moment in Time
Ultimately, the snapshot is an app that providers are using—and they’re using it because we are making their jobs easier and more efficient. They’re no longer searching through extensive documents to find information; they’re opening a tab that sits alongside the others they open every day.
That’s at the heart of Hixny’s identity: we’re a health information exchange, not a health data exchange. Most people don’t ask for large volumes of data; they want information that is relevant to what they’re doing right now, easily and quickly.
In our first 25 years, Hixny’s taken innovative steps to build ourselves a solid base that serves providers, patients, health plans, and population and public health analysts alike. Now, we can leverage and maximize our position to make a marked impact on patient care quality and cost.
Quality, Cost, Satisfaction: A Look at the Future of Healthcare
In consultation with our focus groups of healthcare providers, Hixny has been able to align our service advancements with the longstanding federal aim to improve quality of care and patient satisfaction, while decreasing the cost of care.
That’s no small feat today. Consider:
90% of the $4.5 trillion in annual U.S. healthcare expenses goes to treating and managing chronic or mental health conditions, according to the CDC.
50% of American adults report having at least one health-related social need (HRSN), such as food or housing insecurity, or transportation difficulties, as reported in a study in the Journal of the American Medical Association.
One of the challenges to practicing evidence-based care, cited in various literature, remains the inability to access complete patient records and results.
As we look to the future of healthcare, Hixny is also looking toward the promise of information technology to advance both broad and narrow fields of understanding available to providers and analysts across the healthcare landscape.
Access
Patients and providers expect that information should show up the same way in all systems, so that it’s clear the source of truth is the same. And Hixny is working to make that so.
Across our patient portal, provider portal and snapshot app, and the data warehouse accessed by analysts, we’re applying the same logic, validating data and running reports the same way, so that the view to each group is the same.
Everything legally available to a patient is visible in the patient portal, in a view that matches their provider’s view of the same information.
Data Integration
Today, providers and care managers are inundated by data from different sources with varying levels of validity and timeliness. Hixny is working to validate all data sources that flow to us.
This effort started with NCQA validation for payer and provider data used to assess HEDIS measures annually. It’s since been expanded to cover HRSN assessment through different processes, asynchronously. In fact, we were the first in the country to have our HRSN data stream validated by NCQA.
And Hixny is looking farther ahead to bring even greater nuance and intelligence to our insights, helping providers and care managers know the next right step without having to dig into routine data themselves.
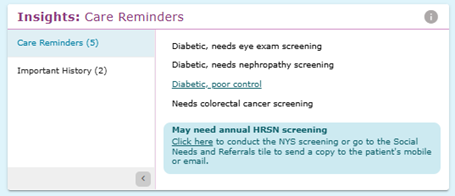
Insights
Expanding beyond our initial insights around blood pressure, diabetes, breast cancer, and colorectal cancer diagnoses and screenings, we’re finding additional ways to surface actionable, conversation-starting points for providers and care managers:
- BMI with the patient’s category assignment (underweight, healthy weight, overweight, etc.)
- Depression screening or diagnosis, and follow-up need
- Emergency or inpatient visit in the past 6 months
For care managers, we’re going deeper, to aggregate these sections with additional information across snapshot and make them downloadable in a PDF. The goal is for that single document to contain all of the information needed to qualify a patient for services, along with a transparent presentation of the data sources behind the insights, information, and recommendations.
Evidence-Based Recommendations
What happens, though, when a patient’s broader health history adds complexity to those insights? That’s the question we’ve been exploring with our collaborators at Ellenville Regional Hospital.
In some cases, important nuances indicate that a patient is at higher risk to develop a condition, and may need more or different screenings, sometimes sooner than general guidelines recommend. For example, if a patient has a high risk of developing breast cancer, it may be appropriate for them to begin mammography screenings earlier than age 40. Surfacing details like this can facilitate a request for consent to participate in the screenings.
The inverse also applies. For example, if a patient has had a preventive bilateral mastectomy due to a high risk of developing breast cancer, a mammogram isn’t indicated. Nor is a cervical cancer screening in a patient who already had a full hysterectomy.
The provider needs to see these nuances in context, with verification of who reported the procedure and results, so they can focus their attention on other issues. This helps avoid uncomfortable conversations and signals to the patient their providers are informed of their full medical history.
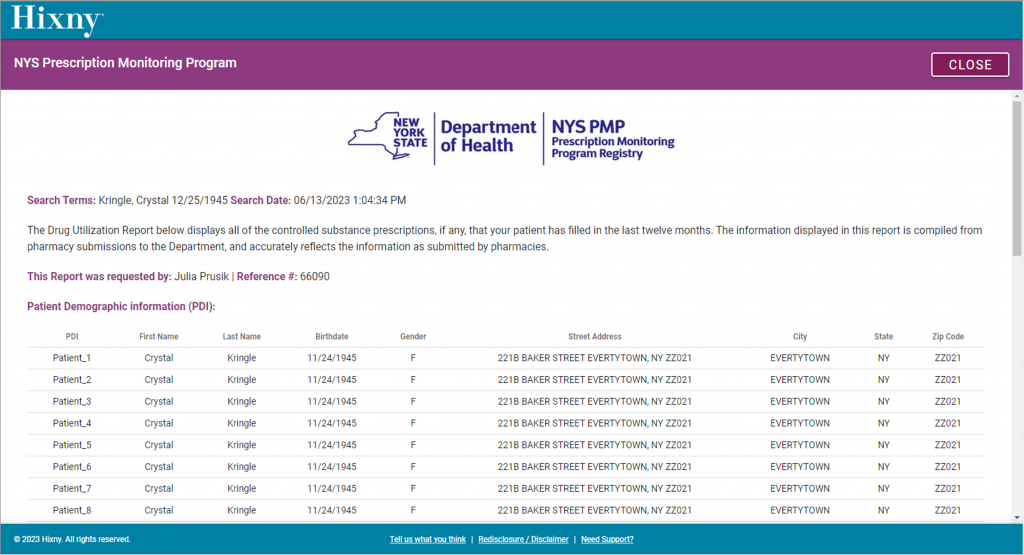
One-Stop NYS Connection
Traditionally, New York’s PMP (prescription monitoring) and PSYCKES (mental health history) databases are not mixed with clinical sources. But the claims data and condition and behavior indicators they contain do improve provider decision making.
Hixny is working closely with the state to allow access to this information alongside our snapshot inside providers’ EHR systems, easing the process of weighing this critical information into encounters and treatment plans. In 2024, we established the connection with PMP (formerly I-STOP), meaning when a provider is looking at a patient’s community record through the Hixny application in their EHR, they can click to access that patient’s controlled substance prescription history.
We are working with the state to understand if a connection to PSYCKES, and therefore access to behavioral health diagnoses and care history, is also possible.
HRSN Care Integration
In another collaboration with the team at Ellenville Regional Hospital, we are exploring ways to integrate not only our HRSN assessment and referral tools into the provider’s snapshot view, but the history of those actions and results into the patient’s record.
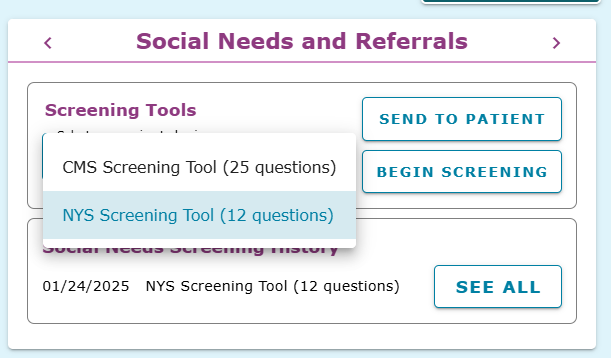
Ellenville initially helped pilot functionality in 2024 to allow for the proactive collection of HRSN data by offering two ways for patients to receive screening questions directly by email or text. Either a doctor could send the patient a link to complete a screening with the click of a few buttons in snapshot or the patient would receive the link automatically when admitted to the emergency room or for inpatient services.
At the end of 2024, in advance of the start of New York’s 1115 waiver requirements, we gave every provider connected to Hixny—either through the EHR embedded snapshot application or through our standalone web-based portal—the ability to use the state-approved, Medicaid-required assessment within the snapshot. Providers can also view all previously collected responses.
The next step is to collect results and gather the outcomes from community-based organizations and make that information available through the snapshot.
As a bonus, the framework Hixny developed for the HRSN assessment can be applied to any screening tool any state entity may require in the future, easing the process of integration.
A Look Ahead
With the patient record snapshot and the patient portal in wide use across eastern New York, we’re expanding our view for 2025 to include a patient dashboard at the population health management level.
This aggregate view for providers and their support staff will also use SMART on FHIR technology to make the dashboard available in EHRs that accommodate contexts beyond individual patient records.
One of the benefits is the ability to set alerts based on any activity within a patient panel. For example, a COPD therapist can choose to receive an alert when anyone on her patient panel visits the ER or is admitted as an inpatient. She can respond in the middle of the night to confer with hospital staff about safe therapy for that patient.
Each of the steps above brings Hixny one step closer to our goal of reshaping the expectations the healthcare world has for information exchange. And in the process, we’re contributing to the continuous improvement of patient care, costs, and satisfaction.
What’s Next for Health Information Technology?
Looking out a number of years, it’s inevitable that various types of healthcare organizations will figure out how to exchange information with each other directly. We’re already seeing cross-customer electronic health records (EHR) sharing through some systems, as well as the development of national networks.
So where does that leave the relevance of health information exchange (HIE)? The short answer is it depends. The long answer is it depends if the organizations providing HIE—like Hixny—are willing to make the changes required to remain relevant.
There’s more and more data coming online every day—not just more organizations, and not just clinical data. For example, health-related social needs (HRSN) data is exploding in utility and importance. And of course, there’s still room for growth in the availability of both clinical and claims data. And one specific data set doesn’t provide a comprehensive view.
Enter HIE, where the role of an organization like Hixny is to bring together data that exists in and beyond the EHR—from and for health plans, providers, public health analysts, HRSN services, and more—and convert it into information that’s available and actionable to the parties that can use it.
New York State’s Medicaid 1115 waiver is a demonstration of the application of this information we anticipate seeing in the future. It introduced two different concepts: HRSN limiting optimal health outcomes, and the possibility for new types of payment models to drive future savings. With healthcare costs on an unsustainable trajectory, a new value-based care (VBC) model incorporating HRSN solutions is a logical path to explore. Hixny already delivers the solid information and insights that providers need to make decisions to drive the VBC model and the surrounding population health approach.
We’ve moved far beyond the days when an HIE was simply an efficient alternative to the fax. We’re bringing together data we have, can access, and can get from our peers statewide. Then, we’re using next-level development to surface insights that draw on all of that data.
Eventually, we can see a day when we deliver the insights alone, because the user no longer needs to dig through the supporting data. That’s why we’re building our capabilities and leveraging technology efficiently to meet the growing demand for meaningful, actionable, decision-supporting information.
